Breast Cancer in North America: Barriers to Prevention and Treatment in Canada, the United States, and Mexico
Breast Cancer in North America: Barriers to Prevention and Treatment in Canada, the United States, and Mexico
Pablo Ashi [1], Srinikha Chejerla [2], and Dr Lopamudra Das Roy
[1]: 1st Author, [2]: 2nd Author
Published: October/2023
@BreastCancerHub, All Rights Reserved
Abstract
Breast cancer is one of the most prevalent cancers globally, and it affects both women and men. One of the biggest risk factors for breast cancer is geographic location; incidence and death rates are largely influenced by the country, province, and/or state one lives in. This research aims to examine the differences or lack thereof in the state of breast cancer across the countries of North America: Canada, the United States, and Mexico. To culminate this review, a wide variety of sources were analyzed including those from the National Library of Medicine, government websites, and cancer societies. Statistical analysis tools were used to produce and reproduce graphs and tables, but the main focus of this research was to gather insights from existing literature and narratives. Although on the same continent, it has been found that there are vast disparities across and within North American countries, with the main issues involving unequal access to healthcare, problems with affordability, and the lack of awareness causing low participation. These are largely driven by the specific healthcare system of each country, its geography, the risk factors of the racial and ethnic populations living there, and access to quality treatments and research. These findings have found that there is still work to be done to educate others on the importance of early detection and ensure that everyone has the opportunity to afford and obtain appropriate treatment for breast cancer.
Canada
Introduction
With Canada’s population of 39 million, breast cancer ranks as the second most common type of cancer. Characterized by free healthcare, the country provides equitable, low-cost care but has long wait times and provincial disparities. This part of the study highlights the current state of breast cancer in Canada including demographic distributions, treatment quality, and needed improvements. It has been found that Canada's breast cancer treatment is advanced, but health inequities across its ten provinces and three territories must be addressed, especially for at-risk groups who have low screening and treatment participation. There are problems with time efficiency, drug insurance coverage, and knowledge gaps.
Prevalence, Mortality, and Distributions
There are no recently reported statistics regarding Canadian breast cancer prevalence, but the last prediction was for 2022: about 28,600 women will be diagnosed with breast cancer, representing 25% of all new female cancer cases. Comparatively, the impact on men is rather minuscule; about 270 men will be diagnosed, representing about .22% of all new male cancer cases. Out of these, an estimated 5,500 women will die, 14% of all female cancer deaths, as well as 55 men, .12% of all male cancer deaths [1,2]. To put this impact into a broader perspective, about one-fifth of all tumor diagnoses in Canada between 1992 and 2017, a 25-year span, were breast cancer-related, as seen in the pie chart. Additionally, the current breast cancer mortality rate in Canada is about 18% [2], an almost 50% decrease since 1986 [3] due to advancing therapies and increased awareness.

In examining age groups, about 83% of cases are among Canadian women aged 50 and above [4]. For this, the Canadian Task Force on Preventive Health Care recommends that women aged 50-74 should receive a mammography screening every 2-3 years [5]. “Risk-stratified screening” is used for those with other risk factors (family history, the BRCA gene, breast density, and hormonal and lifestyle factors) in which they may start earlier [1,3]. In terms of provinces, some disparities are seen. In 2019, Alberta had the highest incidence rate of female breast cancer, with 139 cases per 100,000 females, while Ontario had the lowest, with 133.2 cases per 100,000 females [6].
Canadian Medicare
Canadian Medicare is Canada’s publicly funded, universal healthcare system. It was established in 1984 under the Canadian Health Act which proposed five criteria: it was to be publicly administrated, comprehensive, accessible, universal, and portable [7]. Comprehensibility means that insurance is provided within all health services, accessibility prohibits user fees for publicly-funded treatments, universality ensures standardized terms that prevent preferential treatment, and portability allows coverage for citizens traveling across all territories.
To achieve these goals, Canada’s healthcare system is mainly controlled under the jurisdictions of its 13 provinces and territories; each has its own insurance plan, funds its physicians and programs, controls what services and drugs are provided, and receives aid from the government on a per-capita basis [8]. In addition to free healthcare, two-thirds of Canadians have private insurance to cover supplemental services such as vision and dental care, outpatient prescription drugs, rehabilitation services, and private hospital rooms [9].
There are also several healthcare agencies including Health Canada, the Public Health Agency of Canada, and the Federal Minister of Indigenous Services [8,9]. Health Canada regulates food, drugs, medical devices, and services, Public Health Agency of Canada oversees public health, emergency preparedness, and disease control, and Federal Minister of Indigenous Services specializes in funding health services for the Inuit and First Nations [8].

Advantages of Canadian Healthcare on Breast Cancer
Canada has a high per-capita utilization of procedures [10]. This means that a large number of medical interventions are being performed per person within the population, signifying that individuals can receive necessary procedures without significant barriers. Canadian Medicare is advantageous in accommodating lower-income individuals which allows for higher survival rates than in other countries [11]. For example, it is found that low-income Canadians are at a greater advantage than those <65 years of age who are not eligible for Medicare in the USA [12,13]. While the survival rates of middle and high-income individuals do not significantly differ, those with low-income are more likely to survive 5 years after breast cancer diagnosis [12].
On top of the existing systematic advantages of Canadian Medicare, the country continues to develop its guidelines on breast cancer screening that focus on prevention. The Canadian Task Force recently released their June 7th newsletter suggesting that they may change their every 2-3 years screening suggestion to begin at age 40 rather than 50, following the same guidelines as the US. Their next update has been expedited to fall, 2023 [14].
Disadvantages of Canadian Healthcare on Breast Cancer
Canada's healthcare system faces several challenges and disadvantages that affect breast cancer care including long wait times, utilization of primary providers, the lack of drug insurance, and participation in mammography screening. These are all exacerbated by the presence of disparities among provinces and territories in which some aspects are worse in some places compared to others.
Long Wait Times and Delayed Diagnoses
A high utilization of procedures with limited inpatient beds, operating rooms, and imaging availability leads to both long wait times and lengthy hospital stays [10]. On top of low resources, Canada has about 2.5 physicians per 1000 population which is lower than other countries like the US with 2.6, the UK with 2.7, and Germany with 4.1. Thus, getting an appointment can be a hassle, and an estimated 37% of Canadians can get an appointment with their primary care doctor within 48 hours [10]. Referring someone for a second appointment can be a larger inconvenience; since 2014 there has been a median of 35 days between the time of breast cancer diagnosis and the first round of treatment [15].
A consequence of long wait times is the increasing resistance to medical care due to the inconvenience of getting appointments. Canada is notable for its low rate of citizens with a regular healthcare provider; in 2019, only 14.5% of Canadians aged 12 and above, about 4.6 million people, reported that they did not have a regular healthcare provider [16]. To alleviate this issue, it is important that Canada works to reduce unnecessary procedures and tests as well as further prioritize prevention in order to diminish the toll of medical interventions.
Lack of Drug Insurance Plan
Although Canada’s health care is publicly funded, it lacks a national drug insurance plan which creates disparities among which drugs, especially take-home cancer drugs, “THCDs,” are added to this funding. This is a two-part problem: the process of adding a drug to the public formulary is strenuous and there are provincial disparities on which are insured [7].
The government covers cancer medications administered in a hospital setting, but covering THCDs, mostly oral medications, is unpredictable. This depends on the individual’s province, income, ownership of private drug insurance, and other demographics. As a result, a large portion of the expenditures associated with THCDs typically falls on the individual, making them likely to resist taking the drug or having it at all. For a drug to be approved for public coverage, there is a process of assessing for efficacy, going through a health technology assessment, pricing negotiation, and provincial approval. This takes about 363 days for at least one territory [7].
The second-half of the problem is the inequality amongst provinces and territories of what types of treatments are insured. The table below shows the varying guidelines across Canadian borders. “Exception Status” is an application to be covered by a drug if the person meets proper indications, like low-income. However, this process is lengthy and only lasts around 4-12 months depending on the province. Although 61% of oncologists reported having access to a drug access navigator, 18% of them spent >10 hours per week seeking drug coverage [7]. This taxing process to approve THCDs takes medical professionals away from effectively treating breast cancer and can decrease the quality of care.

Low Breast Cancer Screening Participation
Although Canadian Medicare stresses breast cancer prevention through routine mammography screening, participation is still lower than ideal: about 62.2% in 2018-2019 [15]. The national target is ≥70%, and this low number can be attributed to simple idleness or risk factors of disadvantaged or minority population groups such as those with low-income, other chronic conditions or disabilities, new immigration status, and residencies in remote geographic locations. An article [17] gathered evidence from 29 studies to compile at-risk demographic groups as well as their main challenges to screening and displayed them in the graphs below.

On the left, low socioeconomic status and comorbidities (co-existing conditions), had the greatest prevalence among the studies for significant disparities in screening. These groups have other obstacles to deal with, so committing to routine mammography can be a challenge. Moving to the right, knowledge gap, language barrier, transportation, and low priority were the biggest reasons for lack of participation; this conveys a trend of poor education of breast cancer, reducing the stigma and stressing screening for prevention can help resolve the knowledge gap and make it a higher priority. Language barrier calls for linguistically-trained providers, and transportation requires better infrastructure and easier access to screening locations. These are all improvements that require an approach that not only concerns medical practices but also governmental policies and media outreach.
United States
Introduction
With a population of 332 million, breast cancer ranks as the most common type of cancer in the United States. Characterized by vast demographics and a mixed healthcare system that does not provide universal coverage, the country harbors cutting-edge research to treat breast cancer but has exorbitant costs and disparities among demographics. This part of the study highlights the current state of breast cancer in the United States including demographic distributions, treatment quality, and drawbacks in the delivery of care. The treatment breast cancer treatment in the US is advanced, but health inequities across its 50 states must be addressed, especially for at-risk groups who have low screening and treatment participation.
Prevalence, Mortality, and Distributions
In 2020, the latest year for which incidence data is available from the CDC, there were a reported 239,612 female breast cancer diagnoses, representing 30% of all new female cancer cases for that year. About 42,273 of these women died, representing 17.6% of the cases. To put this into perspective, there were about 119 new cases and 19 deaths for every 100,000 women [18]. The impact on men is not as recently reported and considerably less prevalent; there were approximately 2,300 new cases and 500 deaths in 2017 [19]. It is important to acknowledge that the 2020 reports are skewed due to the disruption in data collection from the COVID-19 pandemic.
For 2023, it is predicted that there will be 297,790 new cases of invasive female breast cancer, meaning it spreads to other parts of the body, and 55,720 new cases of female ductal carcinoma in situ, meaning it remains in the ducts that carry milk from the glands to the nipple. Of those with invasive breast cancer, about 43,700, or 14.5%, are predicted to die [20,21]. These numbers follow the incidence trends over the recent years in which US breast cancer rates have increased by an average of 0.4-0.5% annually from 2010-2019. However, the death rate has decreased steadily over the past decades; it dropped by about 43% from 1989-2020. This is mainly because screening and early detection efforts have improved, there is more awareness, and treatments are advancing with more research. Incidence and death rate data can be seen in the graph below [21, 22].

Prevalence can also be observed across different demographics, such as ages, minority groups, and geographical areas, which present those who may be most at-risk. The average age a woman gets diagnosed with breast cancer in the US is ~62 years old [20], but those who receive regular screenings have ~26% lower breast cancer death rates than women who do not [23]. With the goal of prevention, the US Preventive Services Task Force’s new recommendation as of May 9th, 2023 now advises that women aged ≥40 receive biennial screening rather than the previous 50 and above. For women with dense breasts who cannot use a regular mammograph, the Force does not have guidelines for or against additional screening with breast ultrasound or MRI and is calling for more research [24].
There are also significant disparities among racial and ethnic groups. Black women are 40% more likely to die from breast cancer than white women, and they have the lowest 5-year relative breast cancer survival rate of any other group, since about 20% of cases are triple-negative breast cancer, in which cancer cells do not have any estrogen, progesterone, or HER2 protein receptors, making them harder to treat [22]. Furthermore, Hispanic women have a 20% lower incidence rate of breast cancer than other groups but are often diagnosed in late stages, and Asian/Pacific Islander women have the lowest death rates from breast cancer due to diagnoses at localized stages [23]. In the bar chart, it is seen that white and black women have the highest incidence rates, and American Indians & Alaskan Natives have the highest mortality rates.

For geographic areas, looking at the maps below from the CDC, the states with the highest breast cancer rates from 2016-2020 include Vermont, 138.9 per 100,000, North Carolina, 137.6 per 100,000, and Hawaii with the highest, 140.2 per 100,000 [18]. This data reflects the presence of different racial and ethnic populations, North Carolina has a high rate of non-Hispanic Black populations [25], or lifestyle and environmental factors when it comes to breast cancer; the Hawaiʻi Tumor Registry Principal Investigator Brenda Hernandez summarized that diet, tobacco and alcohol use, and other exposures may be the reason why Hawaii has the highest incidence [26]. As for mortality, southern states have the lowest rates mainly due to difficult access to health care from poverty or rural areas. Mississippi has the highest death rate, 23.5 per 100,000 women, which can be attributed to high-risk racial populations, lack of screening and early women, which can be attributed to high-risk racial populations, lack of screening and early detection, mainly agricultural lands, and about a 20% poverty rate [27].


United States Healthcare System
The American healthcare system is a complex combination of both public and private aspects that involve relations between providers, payers, and patients. The bottom line: there is no universal coverage, so most treatments require a form of payment. In 2021, 91.7% of Americans, 327.7 million people, had some form of health coverage leaving 8.3%, 27.2 million people, uninsured. Of the insured, about 64.3% had private health insurance while 35.7% had public [28].
People with private coverage mainly attain it through their employers, about 83%, while the rest is from direct payment to a health insurance company or through the Affordable Care Act (ACA) marketplace [29,30]. The ACA marketplace is financed by the government which offers premium subsidies, or financial help, to low-income individuals who are not yet eligible for public coverage programs [31]. Private coverage varies depending on the type of company and plan and can have high rates that make them largely inaccessible.
On the other hand, the main forms of public coverage the US government offers are through programs including Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP) [32]. Medicare, covering 18.2% of Americans, provides universal coverage to those ≥65, with long-term disabilities, and/or with end-stage renal disease. Medicaid, covering 17.9% of Americans, gives states health funding for low-income, blind, and/or disabled individuals. CHIP, covering over 9.6 million children, and is a state-administered program for children from low-income families who do not qualify for Medicaid but can’t afford private insurance [30,32].
These mixed systems of coverage make United States breast cancer care costly and largely unequal. Below is a graphic describing the organization and flow of funds within the system.

Advantages of United States Healthcare on Breast Cancer
The United States Healthcare System boasts a range of distinct advantages that position it as a leader in breast cancer care. One lies in its state-of-the-art medical facilities, which offer patients access to cutting-edge technology and advanced treatment modalities [33]. This enables healthcare providers to offer the latest and most effective interventions, contributing to improved patient outcomes. Comprehensive breast cancer screening programs stand as another pillar of the system's strength. The United States places a significant emphasis on early detection through such initiatives, ensuring that breast cancer is identified at its earliest stages when treatment is most effective [34]. This proactive approach plays a pivotal role in increasing survival rates and enhancing overall patient well-being. Furthermore, the United States is a leader in research and innovation within the realm of breast cancer care. Patients benefit from access to groundbreaking interventions that can tailor treatment plans to their specific needs and characteristics. The multidisciplinary care approach is a hallmark of the U.S. healthcare system, wherein collaboration among various medical specialists ensures that breast cancer patients receive holistic and tailored treatment strategies [35]. This comprehensive approach addresses the physical, emotional, and psychological aspects of breast cancer care, ultimately improving patients' quality of life. As mentioned earlier, robust clinical trial infrastructure stands as a testament to its commitment to pushing the boundaries of medical knowledge and treatment. Patients have the opportunity to participate in cutting-edge clinical trials, providing access to experimental treatments and contributing to the advancement of breast cancer care on a global scale. In conclusion, the United States Healthcare System's advantages in breast cancer care span from its advanced medical facilities and comprehensive screening programs to its pioneering research efforts, multidisciplinary care approach, and robust clinical trial opportunities. These advantages collectively showcase the system's commitment to providing patients with the highest quality care and driving continuous advancements in breast cancer treatment.
Disadvantages of United States Healthcare on Breast Cancer
Despite elevated healthcare spending, the U.S. grapples with lower life expectancy and outcomes relative to its counterparts. Noteworthy preventive measures like breast cancer screening, as mentioned before, advocate doing so, yet alarming rates of hospitalizations from preventable causes and avoidable deaths persist. Addressing these issues necessitates cost reduction initiatives, management of risk factors, and promotion of effective care. Substantial private spending and elevated out-of-pocket expenses characterize the U.S. healthcare landscape [36]. While certain aspects exhibit strength, the healthcare system confronts challenges in outcome optimization and cost containment. Among these, the United States stands out with remarkably high private spending and out-of-pocket expenses compared to the other countries. According to the OECD iLibrary US has a high level of public spending, the disproportionately high private spending and out-of-pocket costs contribute to its total healthcare expenditure being much greater than most other OECD nations. This funding structure in the US can lead to financial burdens for individuals, limiting access to care for some populations and highlighting the need for comprehensive healthcare reform to address these disparities and control excessive spending. [37]

Mammography-based breast cancer screening, although effective in early detection, introduces challenges such as overdiagnosis and false positives, potentially leading to unnecessary treatments and anxiety. The American Cancer Society highlights concerns about the financial and access disparities that socioeconomically disadvantaged women and recent immigrants may encounter in accessing optimal breast cancer care, accentuating the need for improved outreach and support programs. Surgical procedures and radiation therapy can result in lymphedema, a distressing arm swelling, underscoring the potential for post-treatment complications impacting patients' well-being [37, 38, 39].
Mexico
Preface
Due to the scarcity of resources and information available on breast cancer in Mexico, there is not a substantial amount of data concerning the prevalence, healthcare system, advantages, and disadvantages compared to the other countries in North America. For this, further research is required in order to gain a deeper understanding, and this section is structured differently.
Introduction to the Mexican Healthcare System
In 1917, shortly after the Mexican Revolution, Mexico adopted its constitution that outlined policies encompassing health, education, and labor. However, due to internal civil conflicts, the effective implementation of a healthcare system was paused. In 1943, Mexico's president established two institutions responsible for the country’s healthcare: The Ministry of Health and The Mexican Social Security Institute (IMSS). The Ministry of Health caters to those not covered by IMSS. This becomes particularly significant in Mexico's socioeconomically disparate landscape, where 1% of the population controls 40% of the wealth [40, 41].
There are 2 different systems in Mexico’s healthcare: public and private. Public healthcare is managed by either the IMSS or Seguro Popular systems. Both offer coverage for medical services and prescriptions, but the system has switched between the two over the years. Seguro Popular ("Popular Health Insurance" in English) replaced the IMMS in 2003 for a better healthcare system, but in 2020, Seguro Popular was changed back to IMSS again due to corruption in the system. No matter the system, people might find navigating the Spanish-language application process challenging, and while public healthcare is generally good, varying service quality and wait times exist. Many people prefer the better-equipped and English-friendly private sector, financed through private insurance, for faster and specialized non-emergency treatments [42, 43].
In 2020, breast cancer accounted for nearly 13% of deaths in Mexico, translating to about 16.38 million cases out of 126.7 million people [44, 45]. In recent years, Mexico has grappled with a pressing issue—the inadequate availability of cancer medicines. The deficiency in information concerning breast cancer compounds the broader challenge of restricted medicine access in the country. Both public hospitals and private pharmacies need to enhance the availability of cancer medicines to align with the World Health Organization's (WHO) target of 80% accessibility [45].
LMICs, Socioeconomic Challenges, and Intervention Solutions
Since 2006, breast cancer has surpassed cervical cancer as a prominent health concern in Mexico. Despite underreporting, detection data reveals a notable shift: while there were around 6,000 new cases recorded in 1990, projections indicate a rise to over 16,500 new cases annually by the year 2020 [46]. Between 1970 and 2021, Mexico witnessed a concerning increase in the breast cancer death rate from 5.22 to 9.65 per 100,000. While routine mammograms are utilized, this is not true in the low-income sectors in Mexico [46].
Disparities are seen in the incidence and mortality rates of cancer within low and middle-income countries (LMICs). As a result, socially disadvantaged cancer patients experience reduced quality of life and shorter survival compared to the wealthy. The WHO defines health inequalities as systematic disparities in the health status among various population groups, leading to adverse social and economic impacts on individuals and societies [47,48]. Social and economic impacts can significantly influence the timeliness of breast cancer diagnosis, and disadvantaged individuals inevitably encounter barriers that lead to delays in seeking healthcare services [49, 50].
However, there are solutions for healthcare and breast cancer care in LMICs like Mexico. The first systematic research was conducted on LMICs, to improve the time of conducting treatment for breast cancer. To analyze available evidence regarding the effectiveness of interventions designed to enhance the timely diagnosis of symptomatic breast and cervical cancers in LMICs, studies have concentrated on the three key stages delineated by the WHO framework: raising cancer awareness and facilitating access to healthcare, utilizing clinical assessment, diagnosis, and staging, and ensuring access to treatment [51, 52]. Unfortunately, there were no results addressing the three key stages.
Disadvantages of Mexico Healthcare & Treatment Delays
As mentioned before, Mexico is currently experiencing a transformation in its healthcare system, the Seguro Popular is shifting to the creation of the IMSS. This reform is relevant, the shift was to eliminate corruption in Seguro Popular, which created problems in breast cancer care; the median period between breast cancer diagnosis to the beginning of treatment is roughly 7 months [53, 54]. This delayed treatment is due to factors like financial constraints, time limitations, fear, and inadequate information. In a 2019 study involving 592 patients with symptomatic breast cancer from two major public cancer hospitals in Mexico City, the association between young age and diagnostic delay of breast cancer (BC) was explored. The Kaplan-Meier curves in the graph below illustrate that women aged ≤40 experienced notably longer diagnostic intervals compared to older women, about 103 days compared to 57 [55].
Addressing this issue involves the implementation of various solutions, one of which is programs like the Free Public Gynecological Cancer Program (FPGC). The FPGC aims to provide accessible and free healthcare services specifically targeted at the early detection, diagnosis, and treatment of gynecological cancers, particularly breast cancers. The program was designed to address the gaps in healthcare access and reduce the burden of these cancers among women, especially those with limited financial means or without social insurance coverage [56]. Unfortunately, there is a lack of awareness about resources such as this, which calls for increased education in Mexico.

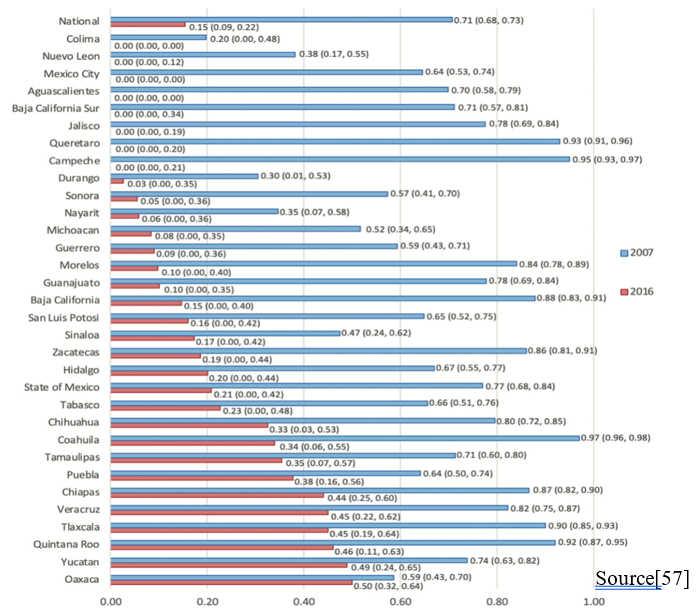
Another study investigates the reduction of the treatment gap from 2007 to 2016 on a state-by-state basis. The bar graph below illustrates a reduction in these years for breast cancer patients who were eligible for financial coverage under the Seguro Popular and FPGC in Mexico. The graph displays red bars representing the estimated treatment gaps in 2007, juxtaposed with blue bars representing the estimated treatment gaps in 2016. Notably, the treatment gap was fully closed in 8 states and demonstrated varying degrees of reduction in 22 out of the 32 states. It's worth noting that Tlaxcala and Quintana Roo lacked cancer centers by the FPGC. The reductions in most states were attributed to improved in-state access, with the exception of the State of Mexico, Morelos, and Hidalgo, where 70 to 80% of patients received treatment in Mexico City [57].
Another disadvantage is the disparity involving health insurance coverage. The graph below provides insight into Mexico's 2018 health insurance landscape, showing the proportions of the population covered by different schemes before Seguro Popular's discontinuation in 2020. Arrows between categories A and B represent affiliations shifting due to labor market and family employment changes. "Nonaffiliated" individuals (Category A) lacked specific insurance but could enroll in Seguro Popular (C), gaining access to breast cancer treatment via the FPGC. "Social security members" (Category B) were linked to social security institutions, with some receiving FPGC-covered treatment through Seguro Popular, a form of supplementary coverage. The graph illustrates how affiliations and employment dynamics impacted healthcare access, especially breast cancer treatment under the FPGC via Seguro Popular. This study promotes the positive systematic approach to Seguro Popular and the reduction of waiting time of the patients in Mexico [57, 58]. To decrease delays for patients, the common suggestion of raising awareness needs to be expanded. Instead of only promoting mammograms, the message should encourage people to recognize possible cancer symptoms, talk about them with others, and know where to get medical help. To shorten the time it takes to diagnose, the focus should be on improving the quality of care in public clinics and making it easier to get to specialized cancer services [58].

Ethnic Inequality and Indigenous Populations
Mexico has the highest indigenous population in Latin America [59] and harbors ethnic disparities in the coverage of women's healthcare. In a study aiming to understand the perception of Mexican women and healthcare providers on the mechanisms of early breast cancer detection, interviews were conducted with 10 providers and 58 women in five communities in Morelos, Mexico, which has a substantial indigenous population. The results showed that providers lack awareness of current regulations and specific clinical guidelines for detecting breast and cervical cancer, with only a few practicing health literacy and intercultural awareness [60]. On the other hand, the women had vague or inaccurate understandings of early detection. Indigenous women had 27% lower coverage compared to non-indigenous women, indicating a gap of 15.1 percent points. [59]. Both of the studies mentioned earlier highlight that Mexican women, especially the indigenous, suffer worsened health and breast cancer care due to factors such as high poverty, limited access to modern treatments, the lack of decision-making authority, and cultural taboos around breast cancer. It is important to address these structural factors to reduce health disparities and improve access to care, starting with improvements in training to ensure adherence to guidelines. It is also urgent to adopt a culturally relevant approach to enable effective communication and promote health literacy regarding early detection.
Moving forward, further cancer research on indigenous populations in Mexico is essential, delving into the unique challenges and barriers in accessing healthcare services. By identifying and understanding these issues, more targeted and culturally-sensitive interventions can be developed [59,60].
The Need for More Cancer Data in Mexico
In Mexico, essential indicators of health system performance for breast cancer are lacking. This refers to a deficiency in comprehensive and standardized metrics that can effectively measure and evaluate various aspects of the healthcare system's response to breast cancer and the lack of breast cancer mortality rate in all parts of Mexico. [61, 62]. In Mexico, essential indicators of health system performance for breast cancer are lacking. Based on my own interpretation, there appears to be a limited availability of statistical data concerning men and statistical cases and mortality rate of breast cancer. Many of the existing data and journal articles are dated from the late 1990s to the late 2000s. This suggests that there is a gap in more recent and comprehensive information pertaining to men's health. Few articles addressed the change in Mexico's National Health Insurance shift from Seguro Popular to IMSS, which has recently occurred in 2020. There is a notable lack of data regarding breast cancer prevalence among Indigenous tribes and Latina ethnicity across Mexico. This scarcity of information hampers our understanding of the incidence and impact of breast cancer within these specific demographic groups.
Conclusion:
The disparities across North America surrounding healthcare and breast cancer treatments underscore the need for continued research, policy reforms, and initiatives to raise awareness and take away the stigma surrounding prevention. While Canada and the US are at the forefront of groundbreaking breast cancer research, they still suffer inequities and systematic issues that must be resolved in order to ensure access for all populations. Mexico also suffers great disadvantages, but more research is required to appropriately address these issues.
References
[1] Lee, S. (2020). Breast cancer statistics. Canadian Cancer Society.
https://cancer.ca/en/cancer-information/cancer-types/breast/statistics
[2] Brenner, D. R., Poirier, A., Woods, R. R., Ellison, L. F., Billette, J.-M., Demers, A. A.,
Zhang, S. X., Yao, C., Finley, C., Fitzgerald, N., Saint-Jacques, N., Shack, L., Turner, D.,
& Holmes, E. (2022). Projected estimates of cancer in Canada in 2022. Canadian Medical Association Journal, 194(17), E601–E607. https://doi.org/10.1503/cmaj.212097
[3] Canada, P. H. A. of. (2017, September 27). Breast cancer. Government of Canada.
https://www.canada.ca/en/public-health/services/publications/diseases-conditions/breast-c
ancer.html
[4] Kirkham, A. A., & Jerzak, K. J. (2022). Prevalence of Breast Cancer Survivors Among
Canadian Women. Journal of the National Comprehensive Cancer Network, 20(9),
1005–1011. https://doi.org/10.6004/jnccn.2022.7028
[5] Klarenbach, S., Sims-Jones, N., Lewin, G., Singh, H., Thériault, G., Tonelli, M., Doull, M.,
Courage, S., Garcia, A. J., & Thombs, B. D. (2018). Recommendations on screening for
breast cancer in women aged 40–74 years who are not at increased risk for breast cancer. Canadian Medical Association Journal, 190(49), E1441–E1451. https://doi.org/10.1503/cmaj.180463
[6] Government of Canada, S. C. (2022, August 23). The Daily — Cancer incidence in Canada,
2019. Www150.Statcan.gc.ca.
https://www150.statcan.gc.ca/n1/daily-quotidien/220823/dq220823b-eng.htm
[7] Horton, S., Camacho Rodriguez, R., Anderson, B. O., Aung, S., Awuah, B., Delgado Pebé, L., Duggan, C., Dvaladze, A., Kumar, S., Murillo, R., Mra, R., Rositch, A. F., Songiso, M., Sullivan, R., Tsunoda, A. T., Teo, S.-H., & Gelband, H. (2020, May 15). Health system strengthening: Integration of breast cancer care for improved outcomes. Cancer. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7197416/
[8] MacPhail, C., & Snow, S. (2022). Not All Canadian Cancer Patients Are Equal—Disparities
in Public Cancer Drug Funding across Canada. Current Oncology, 29(3), 2064–2072.
https://doi.org/10.3390/curroncol29030166
[9] Tikkanen, R., Osborn, R., Mossialos, E., Djordjevic, A., & Wharton, G. (2020). Canada |
Commonwealth Fund. Www.commonwealthfund.org; The Commonwealth Fund.
https://www.commonwealthfund.org/international-health-policy-center/countries/canada
[10] Martin, D., Miller, A. P., Quesnel-Vallée, A., Caron, N. R., Vissandjée, B., & Marchildon,
G. P. (2018). Canada’s universal health-care system: achieving its potential. The Lancet,
391(10131), 1718–1735. https://doi.org/10.1016/s0140-6736(18)30181-8
[11] Cram, P., Dhalla, I., & Kwan, J. L. (2016). Trade-Offs: Pros and Cons of Being a Doctor and
Patient in Canada. Journal of General Internal Medicine, 32(5), 563–565.
https://doi.org/10.1007/s11606-016-3874-0
[12] McAlister, F. A., Cram, P., & Bell, C. M. (2018). Comparing Canadian health care to that in
other countries: looking beyond the headlines. Canadian Medical Association Journal,
190(8), E207–E208. https://doi.org/10.1503/cmaj.171527
[13] Gorey, K. M. (2009). Breast cancer survival in Canada and the USA: meta-analytic evidence
of a Canadian advantage in low-income areas. International Journal of Epidemiology, 38(6), 1543–1551. https://doi.org/10.1093/ije/dyp193
[13] Gorey, K. M., Luginaah, I. N., Hamm, C., Fung, K. Y., & Holowaty, E. J. (2010). Breast
cancer care in Canada and the United States: Ecological comparisons of extremely
impoverished and affluent urban neighborhoods. Health & Place, 16(1), 156–163.
https://doi.org/10.1016/j.healthplace.2009.09.011
[14] CTFPHC. (2023, June 7). Task Force Expedites Update to 2018 Breast Cancer Guideline –
Canadian Task Force on Preventive Health Care. Canadian Task Force on Preventive
Health Care.
https://canadiantaskforce.ca/task-force-expedites-update-to-2018-breast-cancer-guideline/
[15] Chaudhry, M., Kandasamy, S., Habbous, S., Chan, C., Barisic, A., Faisal, A., Walker, M.,
Haque, M., Sheppard, A., Uri, E., Ashu, E., Schwartz, N., Young, S., & Mccurdy, B.
(2021). Cancer System Quality Index 2021 Ontario Cancer System Performance
Acknowledgements Lead Author Co-Authors Content Development and Analytics Leads.
https://www.csqi.on.ca/sites/csqipub/files/assets/CSQI2021Report.pdf
[16] Government of Canada, S. C. (2020, October 22). Primary health care providers, 2019.
Www150.Statcan.gc.ca.
https://www150.statcan.gc.ca/n1/pub/82-625-x/2020001/article/00004-eng.htm
[17] Zha, N., Alabousi, M., Patel, B. K., & Patlas, M. N. (2019). Beyond Universal Health Care:
Barriers to Breast Cancer Screening Participation in Canada. Journal of the American
College of Radiology: JACR, 16(4 Pt B), 570–579.
https://doi.org/10.1016/j.jacr.2019.02.044
[18] CDC. (2023). CDC - Breast Cancer Statistics. Centers for Disease Control and Prevention.
https://www.cdc.gov/cancer/breast/statistics/index.htm
[19] CDC. (2020, October 14). Male Breast Cancer Incidence and Mortality, United
States—2013–2017 | CDC. www.cdc.gov.
https://www.cdc.gov/cancer/uscs/about/data-briefs/no19-male-breast-cancer-incidence-mortality-UnitedStates-2013-2017.htm
[20] American Cancer Society. (2023, January 12). Breast Cancer Statistics | How Common Is
Breast Cancer? www.cancer.org.
https://www.cancer.org/cancer/types/breast-cancer/about/how-common-is-breast-cancer.html
[21] National Cancer Institute. (2023). Female Breast Cancer - Cancer Stat Facts. SEER.
https://seer.cancer.gov/statfacts/html/breast.html
[22] Giaquinto, A. N., Sung, H., Miller, K. D., Kramer, J. L., Newman, L. A., Minihan, A.,
Jemal, A., & Siegel, R. L. (2022). Breast Cancer Statistics, 2022. CA: A Cancer Journal
for Clinicians, 72(6). https://doi.org/10.3322/caac.21754
[23] National Breast Cancer Foundation. (2023). Breast Cancer Facts & Statistics for 2022.
National Breast Cancer Foundation.
https://www.nationalbreastcancer.org/breast-cancer-facts/
[24] USPSTF. (2023, May 9). Draft Recommendation: Breast Cancer: Screening | United States
Preventive Services Taskforce. Www.uspreventiveservicestaskforce.org.
https://www.uspreventiveservicestaskforce.org/uspstf/draft-recommendation/breast-cance
r-screening-adults
[25] OMH. (2023, February 23). Black/African American - The Office of Minority Health.
Minorityhealth.hhs.gov.
https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=3&lvlid=61
[26] U. H. News. (2020, June 9). Recent data shows most common cancers in Hawaii |
University of Hawaiʻi System News. University of Hawaiʻi News.
https://www.hawaii.edu/news/2020/06/09/2012-2016-hawaii-cancer-data/
[27] HHS. (2021). Mississippi - 2021 - III.B. Overview of the State. Mchb.tvisdata.hrsa.gov.
https://mchb.tvisdata.hrsa.gov/Narratives/Overview/9a62acf8-1ab6-4e9a-b92f-90371101
17e7
[28] US Census Bureau. (2022, September 13). Health Insurance Coverage in the United States:
2021. Census.gov. https://www.census.gov/library/publications/2022/demo/p60-278.html
[29] Borrelli, L., & Masterson, L. (2023, August 23). What Is Private Health Insurance? – Forbes
Advisor. Www.forbes.com.
https://www.forbes.com/advisor/health-insurance/private-health-insurance/
[30] Tikkanen, R., Osborn, R., Mossialos, E., Djordjevic, A., & Wharton, G. A. (2020).
International Health Care System Profiles: United States. Www.commonwealthfund.org;
The Commonwealth Fund. https://www.commonwealthfund.org/international-health-policy-center/countries/united-states
[31] Anthem. (2021). Health Insurance Subsidy - What is it | Anthem. Www.anthem.com.
https://www.anthem.com/individual-and-family/insurance-basics/health-insurance/subsid
y
[32] US Census Bureau. (2021, November 21). Health Insurance Glossary. Census.gov.
https://www.census.gov/topics/health/health-insurance/about/glossary.html
[33] ISPOR. (2022). ISPOR - US Healthcare System Overview-Backgound. Www.ispor.org;
ISPOR.
https://www.ispor.org/heor-resources/more-heor-resources/us-healthcare-system-overvie
w/us-healthcare
-system-overview-background-page-1
[34] What’s New in Breast Cancer Research? (n.d.). Www.cancer.org. https://www.cancer.org/cancer/types/breast-cancer/about/whats-new-in-breast-cancer-research.html
[35] Jin, J. (2014). Breast Cancer Screening: Benefits and Harms. JAMA, 312(23), 2585. https://doi.org/10.1001/jama.2014.13195
[36] U.S. Health Care from a Global Perspective, 2019: Higher Spending, Worse Outcomes? (2020, January 30). Www.commonwealthfund.org. https://www.commonwealthfund.org/publications/issue-briefs/2020/jan/us-health-care-global-perspective-2019#:~:text=The%20U.S.%20outperforms%20its%20peers
[37] Health and Economic Benefits of Breast Cancer Interventions | Power of Prevention. (2023, January 27). Www.cdc.gov. https://www.cdc.gov/chronicdisease/programs-impact/pop/breast-cancer.htm#:~:text=Benefits%20of%20Using%20Proven%20Strategies
[38] Breast Cancer Screening. (2019, June 6). National Cancer Institute; Cancer.gov. https://www.cancer.gov/types/breast/hp/breast-screening-pdq
[39] The American College of Obstetricians and Gynecologists. (2017). Breast Cancer Risk Assessment and Screening in Average-Risk Women. American College of Obstetricians and Gynecologists. https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2017/07/breast-cancer-risk-assessment-and-screening-in-average-risk-women
[40] American Cancer Society. (2023). Cancer Facts & Figures 2023| American Cancer Society. www.cancer.org. https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/2023-cancer-facts-figures.html
[41] MEXICO | Summary. (2020, September 26). Columbia University’s Mailman School of Public Health. https://www.publichealth.columbia.edu/research/others/comparative-health-policy-library/mexico-summary
[42] Villarreal, V. (2022, October 7). Infographic | How Do Mexicans Get Healthcare? Wilson Center. Www.wilsoncenter.org. https://www.wilsoncenter.org/article/infographic-how-do-mexicans-get-healthcare
[43] Healthcare in Mexico: Health insurance in Mexico: Allianz. allianzcare.com. (n.d.). https://www.allianzcare.com/en/support/health-and-wellness/national-healthcare-systems/healthcare-in-mexico.html?_its=JTdCJTIydmlkJTIyJTNBJTIyNzJhODVjNzAtM2UwNy00OWFmLThjODUtZGViODEzMjM2ZGNkJTIyJTJDJTIyc3RhdGUlMjIlM0ElMjJybHR%2BMTY5Mjk3NjYyN35sYW5kfjJfMjYwMzNfc2VvX2JmODBkMTZjM2VlMmM4YmY5ZDc4NzQ2ZGM0YWY0MmNkJTIyJTdE
[44] Mexican Healthcare Systems - Health Care in Mexico. (n.d.). International Citizens Insurance. https://www.internationalinsurance.com/health/systems/mexico.php
[45] Mexico Population and Housing Census 2020 | GHDx. (n.d.). Ghdx.healthdata.org. https://ghdx.healthdata.org/record/mexico-population-and-housing-census-2020#:~:text=The%202020%20census%20in%20Mexico
[46] Moye-Holz, D., Ewen, M., Dreser, A., Bautista-Arredondo, S., Soria-Saucedo, R., Dijk, J. P. van, Reijneveld, S. A., & Hogerzeil, H. V. (2020, May 14). Availability, prices, and affordability of selected essential cancer medicines in a middle-income country – the case of Mexico - BMC Health Services Research. BioMed Central. https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-020-05167-9
[47] Knaul, F. M., Nigenda, G., Lozano, R., Arreola-Ornelas, H., Langer, A., & Frenk, J. (2009). Cáncer de mama en México: una prioridad apremiante. Salud Pública de México, 51, s335–s344. https://doi.org/10.1590/s0036-36342009000800026
[48] Sollozo-Dupont, I., Lara-Ameca, V. J., Cruz-Castillo, D., & Villaseñor-Navarro, Y. (2023). Relationship between Health Inequalities and Breast Cancer Survival in Mexican Women. International Journal of Environmental Research and Public Health, 20(7), 5329. https://doi.org/10.3390/ijerph20075329
[49] Bertha Alejandra Martinez-Cannon, Zertuche-Maldonado, T., Sylvia, Servando Cardona-Huerta, Canavati-Marcos, M., Gabriela Sofia Gomez-Macias, & Villarreal-Garza, C. (2020). Comparison of characteristics in Mexican women with breast cancer according to healthcare coverage. 16, 174550652094941-174550652094941. https://doi.org/10.1177/1745506520949416
[50] World Health Organisation. (2018). Health inequities and their causes. World Health Organization. https://www.who.int/news-room/facts-in-pictures/detail/health-inequities-and-their-causes
[51] Nnaji, C. A., Kuodi, P., Walter, F. M., & Moodley, J. (2022). Effectiveness of interventions for improving timely diagnosis of breast and cervical cancers in low-income and middle-income countries: a systematic review. BMJ Open, 12(4), e054501. https://doi.org/10.1136/bmjopen-2021-054501
[52] WHO report on cancer: setting priorities, investing wisely and providing care for all. (n.d.). Www.who.int. https://www.who.int/publications/i/item/9789240001299
[53] Huerta-Gutiérrez, R., Murillo-Zamora, E., Ángeles-Llerenas, A., Ortega-Olvera, C., Torres-Mejía, G., Huerta-Gutiérrez, R., Murillo-Zamora, E., Ángeles-Llerenas, A., Ortega-Olvera, C., & Torres-Mejía, G. (2022). Patient and treatment delays among Mexican women with breast cancer before and after the Seguro Popular. Salud Pública de México, 64(1), 87–95. https://doi.org/10.21149/12472
[54] Mireles-Aguilar, T., Tamez-Salazar, J., Jose Felipe Muñoz-Lozano, Edna Anakarenn Lopez-Martinez, Romero, C., Platas, A., & C. Villarreal-Garza. (2018). Alerta Rosa : Novel Alert and Navigation Breast Cancer Program in Nuevo Leon, Mexico, for Reducing Health System Interval Delays. Oncologist, 23(12), 1461–1466. https://doi.org/10.1634/theoncologist.2018-0226
[55] Saludpublica.mx. (n.d.). https://saludpublica.mx/index.php/spm/article/view/12472
[56] Unger-Saldaña, K., Fitch-Picos, K., & Villarreal-Garza, C. (2019). Breast Cancer Diagnostic Delays Among Young Mexican Women Are Associated With a Lack of Suspicion by Health Care Providers at First Presentation. Journal of Global Oncology, 5, 1–12. https://doi.org/10.1200/jgo.19.00093
[57] Unger-Saldaña, K., Contreras-Manzano, A., Lamadrid-Figueroa, H., Mohar, A., Suazo-Zepeda, E., Espinosa-Tamez, P., Lajous, M., & Reich, M. R. (2022). Reduction in the Treatment Gap for Breast Cancer in Mexico under Seguro Popular, 2007 to 2016. Health Systems & Reform, 8(1). https://doi.org/10.1080/23288604.2022.2064794
[58] Unger‐Saldaña, K., Ventosa‐Santaulària, D., Miranda, A., & Verduzco‐Bustos, G. (2017). Barriers and Explanatory Mechanisms of Delays in the Patient and Diagnosis Intervals of Care for Breast Cancer in Mexico. The Oncologist, 23(4), 440–453. https://doi.org/10.1634/theoncologist.2017-0431
[59] Armenta-Paulino, N., Wehrmeister, F. C., Arroyave, L., Barros, A. J. D., & Victora, C. G. (2022). Ethnic inequalities in health intervention coverage among Mexican women at the individual and municipality levels. EClinicalMedicine, 43, 101228. https://doi.org/10.1016/j.eclinm.2021.101228
[60] Campero, L., Atienzo, E. E., Marín, E., de la Vara-Salazar, E., Pelcastre-Villafuerte, B., & González, G. (2014). [Early detection of breast and cervical cancer among indigenous communities in Morelos, Mexico]. Salud Publica de Mexico, 56(5), 511–518. https://pubmed.ncbi.nlm.nih.gov/25604296/
[61] Mohar-Betancourt, A., Reynoso-Noverón, N., Armas-Texta, D., Gutiérrez-Delgado, C., & Torres-Domínguez, J. A. (2017). Cancer Trends in Mexico: Essential Data for the Creation and Follow-Up of Public Policies. Journal of Global Oncology, 3(6), 740–748. https://doi.org/10.1200/JGO.2016.007476
[62] Breast cancer survival in Mexico between 2007 and 2016 in ... - the lancet. (n.d.-a). https://www.thelancet.com/journals/lanam/article/PIIS2667-193X(23)00115-1/fulltext